
COVID VACCINES DAMAGE ALL HEARTS, STUDY FINDS
October 2, 2023 in News by RBN Staff
source: blacklistednews
Published: October 2, 2023
SOURCE: IGOR CHUDOV
Scientists measured myocardial 18Fluorine-fluorodeoxyglucose (18F-FDG) uptake. F-FDG has molecular similarity to glucose. However, 18F-FDG does not metabolize like glucose. Therefore, PET scans could detect it, and its presence shows the heart muscle’s abnormally high demand for glucose, indicative of abnormal cardiac function. More about it here.
Conclusions: Focal myocardial 18F-FDG uptake seen on oncologic PET/CT indicates a significantly increased risk for multiple myocardial abnormalities.
Indeed, this is what the Nakahara study finds:
RESULTS
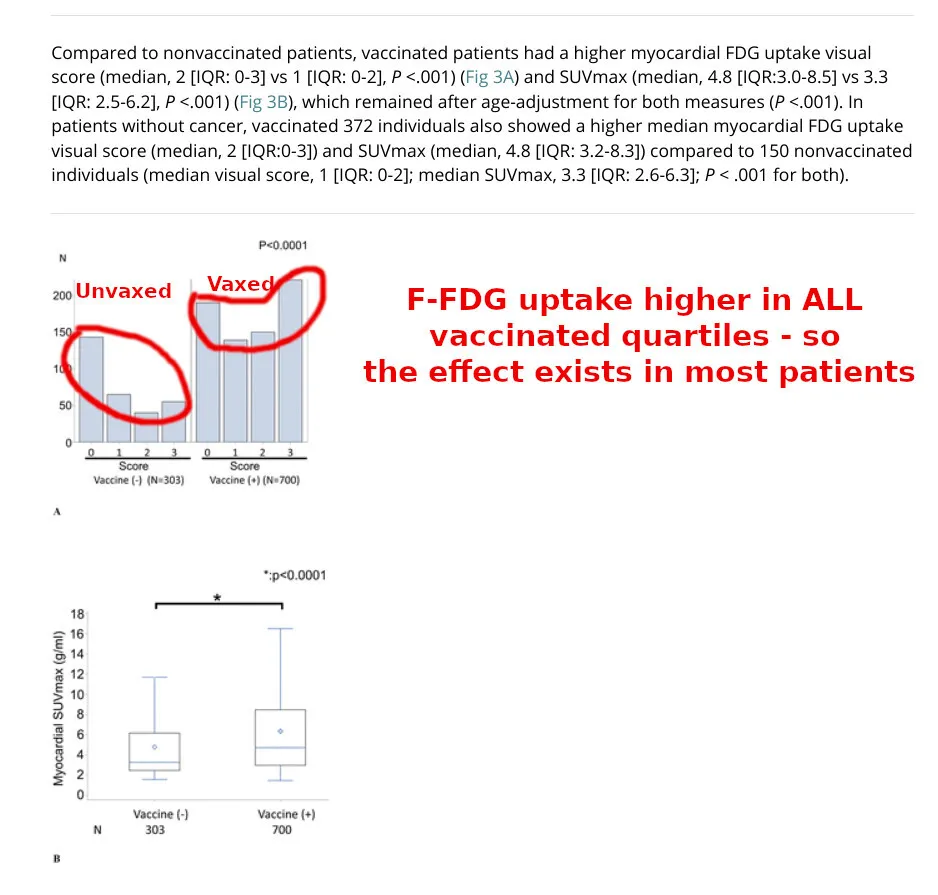
The study included 303 nonvaccinated patients (mean age, 52.9 years; 157 females) and 700 vaccinated patients (mean age, 56.8 years; 344 females). Vaccinated patients had overall higher myocardial FDG uptake compared to nonvaccinated patients (median SUVmax, 4.8 vs median SUVmax, 3.3 ; P < .0001). Myocardial SUVmax was higher in vaccinated patients regardless of sex (median range, 4.7-4.9 ) or patient age (median range, 4.7-5.6) compared to corresponding nonvaccinated groups (sex median range, 3.2-3.9; age median range, 3.3-3.3; P range, <.001-.015). Furthermore, increased myocardial FDG uptake was observed in patients imaged 1-30, 31-60, 61-120, and 121-180 days after their second vaccination (median SUVmax range, 4.6-5.1) and increased ipsilateral axillary uptake was observed in patients imaged 1-30, 31-60, 61-120 days after their 2nd vaccination (median SUVmax range, 1.5-2.0) compared to the nonvaccinated patients (P range, <.001-<.001).
This was not supposed to happen! The COVID vaccine is not supposed to affect the heart in any way. It was promised to “stay in the arm.”
The explosive findings of the study are discussed in the editorial that the editor of the magazine, Dr. Bluemke, felt obliged to publish.
Dr. Bluemke’s editorial is somewhat apologetic, and he gives faint praise for COVID vaccines.
The development of messenger RNA (mRNA) COVID-19 vaccines is a remarkable biotech story. While traditional vaccines took 5-10 years to develop, the COVID-19 vaccines took less than a year. By comparison, the fastest conventional vaccine previously developed was the mumps vaccine, on a timescale of 4 years.
Dr. Bluemke also does not mince words. He explains that the findings are not due to chance:
The main results: asymptomatic patients vaccinated for COVID-19 before PET had about 40% greater radiotracer activity in the myocardium than unvaccinated individuals. The P value was low, less than .0001. This translates to only 1 time out of 10 000 that these results would occur by chance.
The editorial states that there is no rational way to ignore and explain away the negative findings of myocardial inflammation by Takahara et al.:
Vaccine manufacturers are aware of the adverse effects of mRNA vaccines. These adverse effects lead to vaccine hesitancy. The study results by Nakahara et al suggest that mild asymptomatic myocardial inflammation could be more common than we ever expected. This in turn would support a hypothesis of more severe systemic inflammation related to mRNA vaccination in some patients who present with symptoma-c myocarditis.
Dr. Bluemke calls for further research into this:
The investigators understood their first result was only the starting point. They next performed extensive “sensitivity analyses” – i.e., looking at the same data from multiple different directions. What if we account for age differences between groups, and the number of vaccinations? If mRNA vaccinations do cause asymptomatic myocardial inflammation, wouldn’t the effect be more likely shortly after vaccination, rather than 6 months later? Many of us who had COVID-19 vaccines had flu-like symptoms immediately after vaccination – perhaps those of us with common flu-like reactions would have more myocardial inflammation as well? Could trained readers see the differences visually? Or were the differences seen only after placing regions of interest on the heart that could be accidentally mispositioned? The list goes on. Great researchers are also skeptics – they need to prove the results to themselves.
Was the increase in myocardial inflammation due to a few unlucky patients driving high averages, with most people remaining unaffected?
Unfortunately, that is not the case: all quartiles were affected deleteriously, as this image shows:
DOSE-RESPONSE RELATIONSHIP IS PROOF OF CAUSALITY!
Is there a dose-response relationship, providing further proof of causality? Can we see if the higher-dose Moderna vaccine causes MORE heart problems than the lower-dose Pfizer vaccine?
Recall that studies of other topics, such as pregnancy outcomes, show a 42% greater miscarriage rate and 93% greater infant death rate for Moderna (higher dose vaccine) compared to Pfizer.
What about the Nakahara study we are discussing? It shows a weaker but similar pattern of greater response due to Moderna:
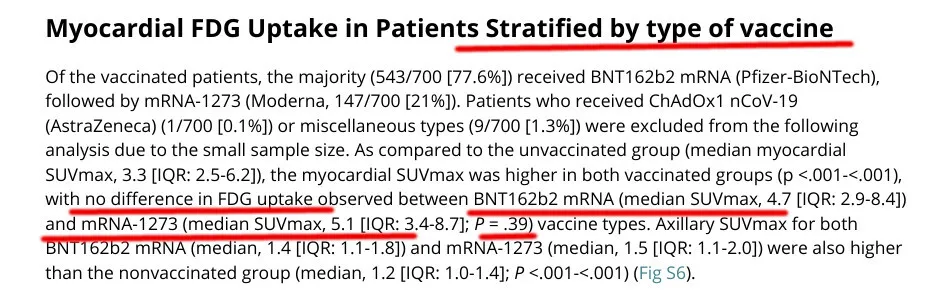
The authors say there is “no difference” between Pfizer and Moderna. However, there IS a difference. Pfizer-vaccinated patients’ SUVmax was 4.7, and Moderna-vaccinated patients (Moderna is a greater dose, remember) had a greater SUVmax of 5.1. The difference did not reach statistical significance, likely due to a small sample size.
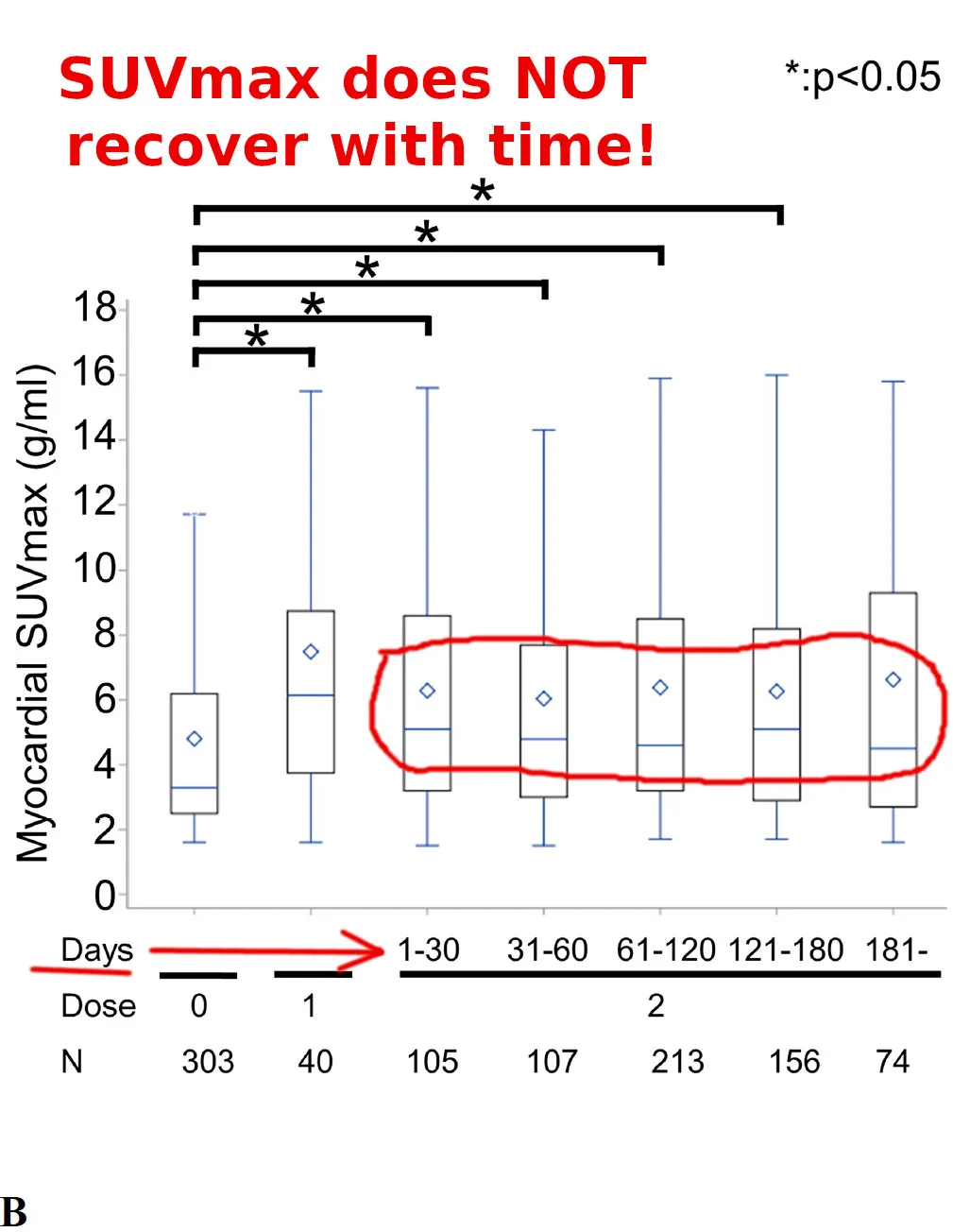
DOES THE ILL EFFECT GO AWAY AS TIME PASSES?
Unfortunately, the scientists’s chart of SUVmax over time does not show complete recovery during 180 days (half a year), still above the unvaccinated level:
THEY COULD HAVE TESTED THIS IS COVID VACCINE CLINICAL TRIALS!
A test of cardiac function via F-FDG uptake, a standard radiological test, is something that careful scientists conducting COVID vaccine clinical trials could carry on with a few hundred patients. Watchful vaccine safety agencies could demand such tests to be conducted to ensure the general public’s safety. They chose not to do it, and their sponsors (Pfizer and Moderna) made much money selling unproven and untested COVID vaccines.
The vaccines, instead of stopping the pandemic, damaged the heart muscles of millions.
I hope that the vaccinated people will be able to ask for compensation for their damaged hearts.
The reality, sadly, is that the damage will most likely be ignored, and the vaccine billionaires will enjoy their newfound wealth while the hysterical Pfizer-sponsored press will be scaring us with new distractions.
What do you think?